
The numbers behind healthcare staffing in 2026 are hard to ignore. The U.S. faces an 8.06% nursing shortage, with RN demand outpacing supply by more than 350,000 full-time positions. Add physician gaps, accelerating AI adoption, and a workforce increasingly vocal about burnout, and the case to track healthcare workforce trends 2026 becomes clear. This guide walks healthcare professionals and analysts through the data sources, monitoring methods, and strategic decisions that separate organizations reacting to shortages from those anticipating them.
Table of Contents
- Key takeaways
- How to track healthcare workforce trends 2026: data sources and metrics
- Steps for monitoring and analyzing workforce trends effectively
- Common pitfalls in healthcare workforce data tracking
- Interpreting trend data into staffing and retention action
- My take on workforce trend tracking in 2026
- How ConnectedMedics supports workforce trend tracking
- FAQ
Key takeaways
| Point | Details |
|---|---|
| Use multiple data sources | Combine HRSA projections, internal HR metrics, and staffing agency reports for a full picture. |
| Segment by geography and role | National averages mask local crises; rural areas face far steeper shortages than metro regions. |
| Track burnout as a leading indicator | Burnout is the top workforce threat in 2026, making morale monitoring a frontline priority. |
| Integrate AI tools deliberately | Nearly half of staffing agencies use AI for recruiting; intentional human-AI design outperforms technology alone. |
| Treat retention as capacity | Every nurse lost costs $40,000 to $60,000 to replace, making retention a financial strategy, not just HR. |
How to track healthcare workforce trends 2026: data sources and metrics
Effective healthcare workforce analysis 2026 starts with knowing where to look. No single data source tells the whole story. HRSA projections give long-range demand forecasts by specialty and geography. Staffing agency reports capture real-time supply shifts, placement rates, and compensation benchmarks. Your internal HR data, when properly structured, reveals what national reports cannot: your specific vacancies, your time-to-fill by unit, and your turnover patterns by role.
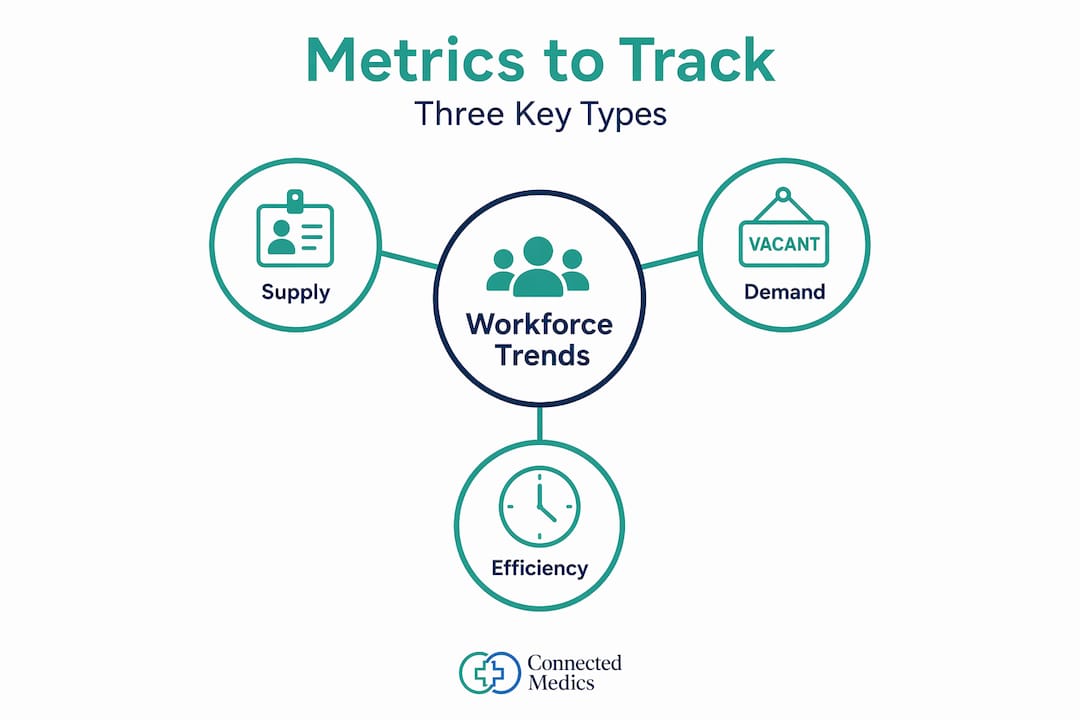
The metrics worth monitoring fall into three categories.
Supply metrics: Active licensed providers by role, credential expiration rates, graduation pipeline volume from regional schools.

Demand metrics: Open positions by unit and care setting, patient volume per available FTE, specialty-specific vacancy rates.
Efficiency metrics: Time-to-fill by role, offer acceptance rates, cost-per-hire, and cost of turnover. Nurse turnover alone runs $40,000 to $60,000 per replacement, which makes this last category particularly consequential at leadership level.
| Data source | What it reveals | Best for |
|---|---|---|
| HRSA workforce projections | Long-term demand by specialty and region | Strategic planning, capital decisions |
| Staffing agency reports | Real-time market rates, supply signals | Competitive compensation benchmarking |
| Internal HR systems | Role-specific vacancy, turnover, and time-to-fill | Operational decision making |
| Certification bodies (NHA, ANCC) | Skills gaps, credential trends | Training investment priorities |
| AI recruitment platforms | Candidate pipeline velocity, decline reasons | Tactical hiring improvement |
Certification data deserves more attention than most systems give it. 89% of employers prefer certified candidates, and 66% report better retention among certified allied health professionals. Tracking credential rates within your workforce and your applicant pool gives you a measurable signal of both quality and likely tenure.
Pro Tip: Set up a monthly data dashboard that pulls from at least three sources: one external (HRSA or a staffing industry report), one operational (your HRIS), and one market-facing (a job posting analytics tool). Single-source tracking creates blind spots that show up as surprises.
Steps for monitoring and analyzing workforce trends effectively
Knowing your data sources is one thing. Building a repeatable process to monitor healthcare job market conditions is another. Here is a practical approach.
-
Segment before you analyze. Break data down by geography, role type, and care setting before drawing conclusions. Rural areas project a 58% physician shortage in nonmetro areas by 2038, while urban academic medical centers face entirely different pressures. A single national number applied to a rural system will produce a plan that fits no one.
-
Track candidate preferences alongside vacancy data. Candidates now prioritize schedule flexibility. Four-day workweeks and hybrid arrangements are increasingly expected, not just appreciated. Organizations that ignore this lose candidates to those that don't.
-
Incorporate AI-enabled tools with clear governance. Approximately 45% of healthcare staffing agencies now use AI-powered tools for recruiting and scheduling. These tools accelerate hiring speed and improve candidate matching, but intentional human-AI collaboration design produces better outcomes than deploying technology without defined workflows. Know what the AI is deciding and what humans are deciding.
-
Watch burnout indicators as early warning signals. Burnout ranks as the top perceived workforce threat at 29% across travel nurses and allied health professionals. Pulse survey scores, PTO utilization spikes, and voluntary overtime declines are measurable precursors to departures. Waiting for exit interview data means the problem left the building weeks ago.
-
Mine granular internal metrics for market alignment. Decline reasons and negotiation trends reveal where your offers are missing the market. If candidates consistently decline citing compensation or call schedules, those patterns are quantifiable and fixable. If you are not tracking them, you are guessing.
| Tracking approach | Traditional method | AI-enabled method |
|---|---|---|
| Vacancy identification | Monthly HR reports | Real-time dashboard with predictive alerts |
| Candidate matching | Manual resume review | Algorithm-driven profile scoring |
| Turnover forecasting | Historical averages | Predictive models using engagement data |
| Credential verification | Manual document checks | Automated credentialing with expiry alerts |
| Compensation benchmarking | Annual salary surveys | Live market rate feeds from job boards |
Pro Tip: Review your offer decline log every quarter. Categorize declines by reason: compensation, location, schedule, benefits. If one category dominates, you have a specific, solvable problem rather than a vague talent shortage.
Common pitfalls in healthcare workforce data tracking
Most organizations track something. Fewer track the right things, and even fewer act on what they find. These are the errors worth avoiding.
-
Relying on national averages without local context. Healthcare labor market changes vary sharply by region. A nationally published RN vacancy rate tells a system in rural Montana almost nothing useful about its own hiring environment. Always apply geographic filters before interpreting any aggregate figure.
-
Counting heads instead of measuring capacity. Headcount is not the same as usable workforce capacity. A unit with six nurses and three on extended leave due to burnout does not have six nurses available. Productivity and availability metrics matter as much as roster size.
-
Ignoring qualitative signals. Survey data, focus group themes, and informal manager feedback capture things that spreadsheets miss. Morale decline and retention risks develop through cultural shifts that show up in conversations before they show up in turnover rates.
-
Failing to segment by specialty and setting. An APRN shortage is not the same as an LPN shortage. A shortage in the ICU is not interchangeable with a shortage in home health. Blending these into a single workforce number produces plans that serve no specific unit well.
-
Skipping certification and career pathway data. Career ladders improve retention for 91% of employers who use them, yet many organizations have no mechanism to track whether employees are progressing along defined pathways.
The most dangerous staffing trap in healthcare is the reactive cycle: shortage detected, travelers contracted, costs spike, leadership reacts, cycle repeats. Breaking this cycle requires treating workforce data as a continuous operational signal, not a quarterly report reviewed at budget time.
Interpreting trend data into staffing and retention action
Data collection is only half the job. Translating 2026 healthcare employment trends into decisions is where most workforce strategies either hold or fall apart.
-
Make retention a capacity decision, not an HR task. Retention directly affects patient care capacity and financial sustainability. Calculate your annual turnover cost, put a dollar figure to leadership, and make the case for retention investment the same way you would make the case for a capital purchase. The math is persuasive.
-
Expand team-based care models. A strategic model that expands LPN and virtual nursing roles reduces bedside RN pressure more durably than reactive hiring alone. Use your workforce data to identify which roles are overextended and which adjacent roles could absorb appropriate tasks.
-
Build local talent pipelines. Partner with community colleges, nursing schools, and allied health programs in your region. Track graduation timelines and class sizes as leading indicators of future supply. This is forward-looking workforce data tracking that most competitors are not doing.
-
Use AI analytics for real-time responsiveness. Organizations integrating people, skills, data, and technology in real time outperform peers in both adaptability and financial results. AI-powered scheduling tools, credential tracking, and candidate pipeline visibility give workforce planners a current picture rather than a lagging one. Connect these to your healthcare vacancy applications process to reduce friction for incoming candidates.
-
Incorporate certification and scope data into hiring plans. Certification correlates strongly with retention and performance in allied health. Build credential requirements and preferred certifications into your job postings and screening criteria. Track the ratio of certified to uncertified hires over time and measure retention by group. Understanding training pathways for healthcare assistants supports this approach from the talent development side.
Pro Tip: Build a quarterly workforce review cycle with three outputs: a red-yellow-green status on each critical role category, one retention action in progress, and one pipeline investment planned. Consistent rhythm beats comprehensive annual reports.
My take on workforce trend tracking in 2026
I've spent enough time working with healthcare organizations to say this plainly: most workforce planning still runs on intuition dressed up as data. Leaders pull a vacancy number, compare it to last year, and call it analysis. That approach is expensive.
What I've found is that the organizations managing workforce risk best in 2026 are the ones treating turnover cost as a balance sheet issue. When you put a real number on what it costs to replace one nurse, $40,000 to $60,000 in recruitment, onboarding, and lost productivity, conversations about retention investment change completely. Finance listens differently when the cost is quantified.
The AI piece also deserves a more honest framing than it usually gets. AI doesn't fix a shortage. What it does is accelerate matching, reduce credentialing lag, and surface signals earlier. The value isn't in automation. It's in speed and visibility. And that only works if the humans using those systems know how to interpret and act on what they're seeing.
My advice to any healthcare leader reading this: stop treating workforce data as something your HR team owns and reviews quarterly. Make it a weekly operational metric the same way you track patient volume or bed occupancy. The data is available. The gap is attention.
— David
How ConnectedMedics supports workforce trend tracking
ConnectedMedics is built specifically for the challenges healthcare professionals and recruiters face when the market moves faster than traditional tools can track. The platform gives recruiters direct access to verified healthcare professionals with confirmed credentials, removing the credentialing lag that slows hiring when vacancies are urgent. With over 4,600 active healthcare roles on the global jobs board, the platform reflects real-time supply and demand in a way generic networks cannot.
For organizations focused on flexible staffing models, the ConnectedMedics marketplace supports hybrid and contract arrangements alongside permanent placements. The Knowledge Hub delivers workforce insights and clinical guidance contributed by verified medical experts, making it a practical resource for ongoing healthcare workforce data tracking. For professionals and recruiters who want a platform aligned with how healthcare actually works in 2026, ConnectedMedics is a direct fit.
FAQ
What are the biggest healthcare workforce challenges in 2026?
Burnout ranks as the top threat at 29%, followed by morale decline and retention issues. Nursing shortages exceed 350,000 unfilled RN positions nationally.
How do I track healthcare workforce trends at the local level?
Use geographic filters on HRSA data, supplement with regional staffing agency reports, and monitor your internal time-to-fill and offer decline data by location and role.
What role does AI play in healthcare staffing analysis 2026?
Roughly 45% of staffing agencies now use AI tools for recruiting and scheduling. AI improves matching speed and candidate pipeline visibility but requires intentional human oversight to produce reliable outcomes.
How much does nurse turnover actually cost?
Replacing one nurse typically costs between $40,000 and $60,000 when accounting for recruitment, onboarding, and productivity loss. Tracking this figure makes the financial case for retention investment at the leadership level.
How does certification data improve workforce planning?
Certified allied health professionals show higher performance and retention rates. Tracking certification in your workforce and applicant pool gives a measurable quality signal that supports better hiring and training decisions.